After three years of phased implementation, the transition from CMS-HCC Version 24 to Version 28 is complete. V28 now governs 100% of Medicare Advantage risk adjustment payments. The organizations that understood this change early are collecting. The ones that didn't are discovering the gap — quietly, in their quarterly reconciliations.
I have spent the past decade on the payor side of managed care. Before that, I practiced emergency medicine — a career that spans the full arc of healthcare from bedside urgency to boardroom strategy. What I have watched unfold with the V24-to-V28 transition confirms something I have believed for years: the gap between clinical quality and financial recognition is not a clinical problem. It is a documentation and infrastructure problem.
V28 did not change the medicine. It changed the rules for how medicine gets counted. And that changes everything about how MA plans, ACOs, and provider groups get paid.
projected by CMS under V28
payment-eligible HCC mapping
from V28 in 2024 alone
What Actually Changed — and What Didn't
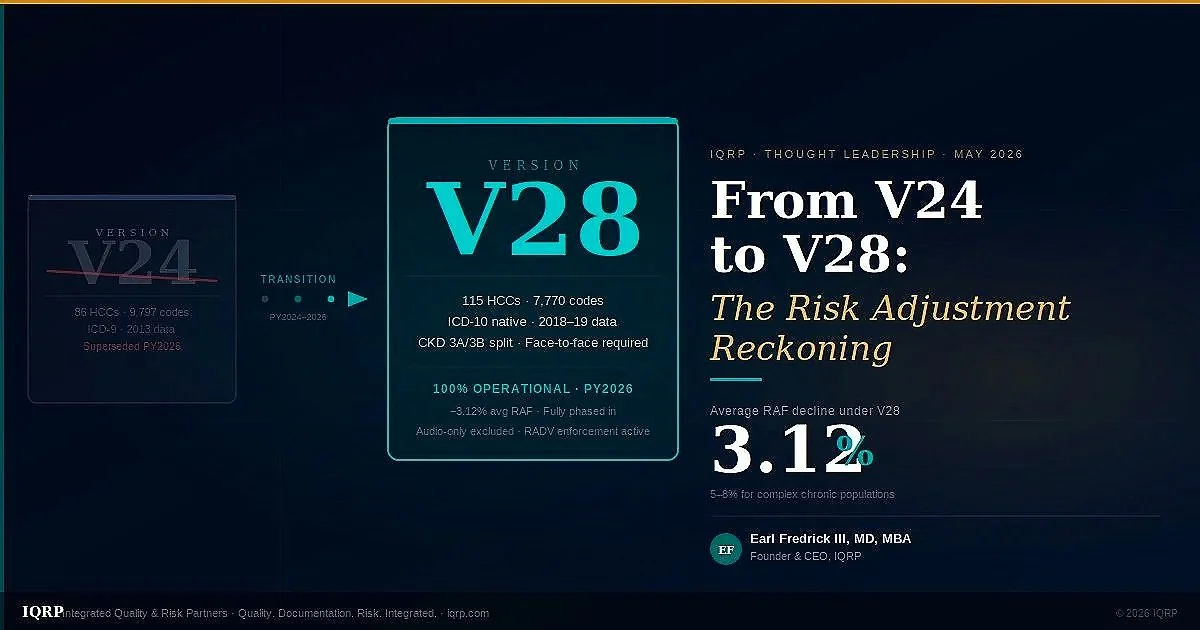
The most important thing to understand about V28 is what it is and is not. It is not an accusation of fraud. It is not a clawback. It is a recalibration of the model used to predict the cost of caring for a Medicare Advantage population — updated from data that was nearly two decades old to data reflecting how FFS Medicare actually spent money in 2018 and 2019.
V24 was built on ICD-9 logic. It had 86 HCC categories capturing 9,797 ICD-10-CM codes. V28 is rebuilt natively on ICD-10, with 115 HCC categories — but only 7,770 valid diagnosis codes. That net reduction of more than 2,000 codes is the headline number, but it understates the real change.
| Dimension | V24 | V28 (PY2026, fully operational) |
|---|---|---|
| HCC categories | 86 | 115 (expanded granularity) |
| Payment-eligible ICD-10 codes | 9,797 | 7,770 −2,294 removed +268 added |
| Calibration data | 2013 diagnoses / 2014 expenditures | 2018 diagnoses / 2019 expenditures |
| ICD-10 native | No (crosswalked from ICD-9 logic) | Yes — direct ICD-10-CM mapping |
| CKD staging | CKD 3 combined (no 3A/3B split) | CKD 3A and 3B now separate HCCs new coefficient split |
| Audio-only visits | Permitted for risk adjustment | Excluded — face-to-face required |
| Avg RAF score impact | Baseline | −3.12% average; −5–8% in high-acuity populations |
| RADV exposure | Extrapolated audits finalized 2023 | Add-only programs explicitly targeted; DOJ enforcement active (Aetna/CVS settlement $117.7M, March 2026) |
| Blended phase-in | — | PY2024: 67% V28 / 33% V24 · PY2025: 33% V28 / 67% V24 · PY2026: 100% V28 |
Why the 3.12% Headline Understates the Real Impact
CMS published the 3.12% average RAF decline figure, and many organizations have anchored on that number. I want to explain why the average is misleading for most of the plans and ACOs I work with.
The average is computed across all MA beneficiaries — including healthy, low-RAF members who are barely touched by the HCC model changes. For medically complex populations — the patients driving 80% of the cost and 80% of the revenue — the RAF compression is far steeper.
Consider a 72-year-old member with CHF, COPD, Type 2 diabetes with complications, and CKD Stage 3. Under V24, each of those conditions contributed to a layered RAF score, with some lower-specificity codes (say, E11.9 unspecified diabetes, I50.9 unspecified heart failure, J44.9 unspecified COPD) generating substantial payment HCCs. Under V28:
E11.9 (DM unspecified) no longer maps to the highest-value HCC in the diabetes hierarchy. E11.40–E11.65 (DM with specific complications) does. I50.9 (CHF unspecified) maps to a lower HCC than I50.22 (CHF, systolic, chronic) or I50.33 (CHF, diastolic, acute-on-chronic). J44.9 (COPD unspecified) maps lower than J44.1 (COPD with acute exacerbation).
In each case, the clinical condition is the same. The documentation is different. And the payment is different. That is not a coding trick — it is an accurate reflection of clinical reality that the old model couldn't capture.
For a population of predominantly complex chronic disease patients — the exact population that MA plans are designed to serve — the real RAF impact of unresolved specificity gaps can be 5–8% or more. At $1,100 PMPM average capitation, that is $660–$1,056 per member per year, multiplied across an entire attributed population.
V28 isn't a technical update to a model. It's CMS signaling that they want documentation to reflect actual patient complexity — not a list of codes accumulated over years of low-specificity encounters.
The Five Conditions That Matter Most Under V28
Not all HCC changes carry equal weight. Based on IQRP's analysis of Tier 1 market populations — concentrated in Tennessee, Texas, North Carolina, Ohio, and Missouri — five condition groups generate the most significant RAF compression and the most actionable recovery opportunity.
1. Congestive Heart Failure
V28 differentiates systolic vs. diastolic failure and acute vs. chronic presentation, with meaningfully different HCC coefficients. I50.9 (unspecified) documents the same patient for less revenue than I50.22, I50.32, or I50.43. In high-CHF markets like Cleveland and Columbus, this is the single largest per-member RAF recovery opportunity. Every encounter with a CHF patient is an opportunity to specify — and most provider EMR systems default to unspecified on auto-populated problem lists.
2. COPD with vs. without Exacerbation
J44.0 (COPD with acute lower respiratory infection) and J44.1 (COPD with acute exacerbation) carry higher coefficients than J44.9. The clinical distinction exists in the chart — spirometry results, symptom documentation, treatment escalation. It just isn't always making it to the claim. Tennessee and Oklahoma have among the highest COPD prevalence in Tier 1 markets, making this a first-priority coding education target.
3. Diabetes with Complications (CKD crossover)
V28 rewards specificity across the diabetes complication hierarchy: nephropathy, retinopathy, peripheral neuropathy, and autonomic neuropathy each map to distinct HCCs when coded correctly. The combination of E11.65 (DM with hyperglycemia) + N18.31 (CKD Stage 3B) captures two separate V28 HCCs where V24 may have captured one or collapsed them. The CKD 3A/3B split is new to V28 and is systematically undercoded because the clinical distinction wasn't previously relevant to payment.
4. CKD Stage 3B (New V28 Split)
This is perhaps the most frequently missed V28 opportunity. CKD Stage 3 was a single HCC in V24. V28 separates it into 3A (N18.31) and 3B (N18.32), with different payment coefficients. Most EHR problem lists from the V24 era code N18.3 (unspecified Stage 3) or N18.30 — codes that no longer map to the correct V28 HCC. The fix requires pulling current eGFR lab values and updating the diagnosis to the specific substage. It is a five-minute chart review with material payment impact.
5. Dementia with Behavioral Manifestations
V28 significantly expanded specificity requirements for dementia — Alzheimer's vs. vascular vs. Lewy body, with vs. without behavioral disturbance, with vs. without psychotic features. The higher-specificity codes carry materially higher coefficients. F01.51 (vascular dementia with behavioral disturbance) vs. F01.50 (without) is a meaningful coefficient difference that reflects actual clinical complexity and cost — but only gets captured if the encounter documentation supports it.
The RADV Dimension: Documentation-First Is Not Optional
V28 does not exist in isolation. It arrived alongside the finalized RADV (Risk Adjustment Data Validation) audit methodology that allows CMS to extrapolate audit findings to the full contract. The Aetna/CVS $117.7 million DOJ settlement in March 2026 is the clearest signal yet of where enforcement is headed.
The DOJ settlement specifically penalized an add-only retrospective risk adjustment program — one that submitted additional diagnosis codes without deleting unsupported diagnoses identified in the same chart review. CMS now requires bidirectional integrity: if a review finds an unsupported HCC, it must be deleted. Add-only programs carry maximum audit exposure.
The implication for IQRP clients is clear: every HCC submitted must be supported by face-to-face encounter documentation reflecting provider assessment of the condition. Chart-review-only HCCs — without a qualifying in-person or synchronous video encounter — represent audit liability, not revenue protection.
The V28 audio-only exclusion compounds this. Telephone encounters, portal messages, and staff-only visits do not satisfy the face-to-face requirement. With the behavioral health workforce shortage driving more care to telephone channels, plans need to audit their EDPS submission pipeline for audio-only CPT codes before they become a RADV finding.
The Transition Timeline — Where We Are Now
What the Best-Prepared Organizations Did Differently
Over the past two years, I have watched some organizations navigate this transition with extraordinary precision and others absorb avoidable losses. The difference was not resources — it was sequencing.
The best-prepared organizations did three things that most did not:
1. They ran a V24-to-V28 crosswalk before the blend began. They identified every condition in their attributed population where the two models diverged, calculated the RAF impact, and prioritized outreach by revenue risk — not by condition prevalence. The list was short. The top 15 HCC specificity gaps drove 70% of the exposure.
2. They invested in EDPS pipeline integrity before coding programs. Retroactive coding means nothing if the encounter doesn't make it to EDPS. They fixed the submission pipeline first — PECOS validation, 999/277CA monitoring, MAO-004 reconciliation — before layering on provider education.
3. They built prospective outreach programs anchored on AWV. The Annual Wellness Visit is the highest-leverage encounter in the V28 world. It creates a face-to-face encounter — satisfying V28's requirement — and provides the opportunity to update chronic condition specificity on every eligible member, annually, as part of normal care workflow.
The IQRP Integrated Response
IQRP was built specifically for this inflection point. Our platform integrates the three components that the V24-to-V28 transition demands: quality infrastructure, documentation integrity, and risk adjustment pipeline management.
Our FHIR-based data engineering layer ingests encounter data, lab results, and pharmacy claims in real time — identifying V28 specificity gaps at the point of care rather than retroactively. Our NLP-driven analytics surface the members and providers where the gap between documented complexity and coded complexity is widest. Our clinical education programs translate the ICD-10 specificity requirements into provider-facing workflows that close gaps without adding documentation burden.
The economic opportunity model we have built for each IQRP client starts from a simple premise: a conservative 2% RAF lift through V28 specificity optimization, at $1,100 PMPM average MA capitation, generates $22 PMPM in additional revenue — every month, every member, compounding year over year as the V28 coefficients become the permanent baseline.
For a plan with 50,000 attributed MA members, that is $13.2 million annually from specificity optimization alone — before accounting for quality bonus payment improvements or LIS auto-enrollment growth from Stars performance.
The Bottom Line for MA Plans, ACOs, and Provider Groups
V28 is not coming. It is here. The transition period is over. The organizations that treated this as a future problem are now experiencing it as a current-year financial reality.
The path forward requires three things acting in concert: a documentation-first clinical program that captures specificity at the point of care; a data pipeline that ensures every qualifying encounter reaches EDPS with the correct diagnosis codes; and a compliance program that protects the resulting RAF claims from RADV exposure.
That is not three separate programs. That is one integrated program — and it is exactly what IQRP was built to deliver.
I founded IQRP because I have lived both sides of this equation — as a clinician who watched quality care go unrecognized, and as a managed care leader who watched documentation failures translate directly into revenue loss. The gap is closeable. The tools exist. The regulatory framework — V28, EDPS, RADV — actually rewards accuracy over volume for the first time in the history of this program.
That is not a problem. That is an opportunity — for the organizations willing to close the gap between the care they deliver and the credit they receive for it.
Earl Fredrick III, MD, MBA is the Founder and CEO of IQRP — Integrated Quality & Risk Partners. He can be reached at efredrick@iqrp.org or 312-523-9681. IQRP partners with Medicare Advantage plans, ACOs, D-SNPs, and PACE organizations to close the gap between clinical quality, documentation integrity, and financial sustainability.